Due to the sad demise of our beloved Dr.Shekhar Agarwal, his dedicated team of surgeons will be available for all your needs, please click on the below surgeon links to book an appointment with them
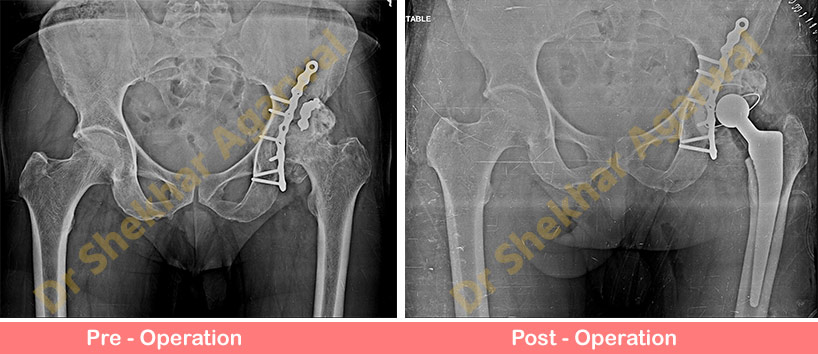
62 years old gentleman came with pain in left hip and difficulty in walking for the past 3 years. He had acetabular fracture which was treated by internal fixation. He could barely walk without support and had restricted movement of the hip. Preoperative x-ray showed arthritic hip with plates in situ. At surgery the plate was penetrating into the acetabulum. Since bone had grown over the plate removal of the plate would have risked the sciatic nerve. Therefore cemented cup was used without removing the plate. The uncemented femoral component was used in the usual manner.
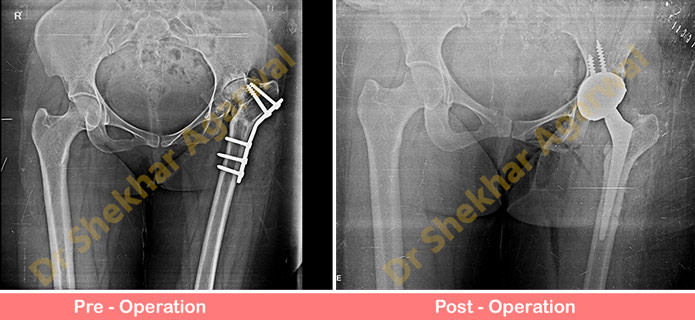
26 years old lady came with complaints of left hip pain, shortening of leg and limp. She had a history of infection in the left hip in childhood following which she developed deformity. She underwent surgery (Valgus Osteotomy) elsewhere (See pre-operative x-ray)
On Clinical examination she had fixed adduction and flexion deformities with minimal movements at the hip. X-rays revealed advanced arthritis of hip joint with implant in situ. All infection markers were negative. We planned for Total Hip Replacement. Doing total hip replacement in these patient is challenging as acetablular socket is deformed and shallow while femoral canal is narrow and not straight to pass the stem easily.
There are associated soft tissue contractures. We used uncemented dual mobility cup, uncemented wagner cone stem with ceramic head. (See post op x-ray)
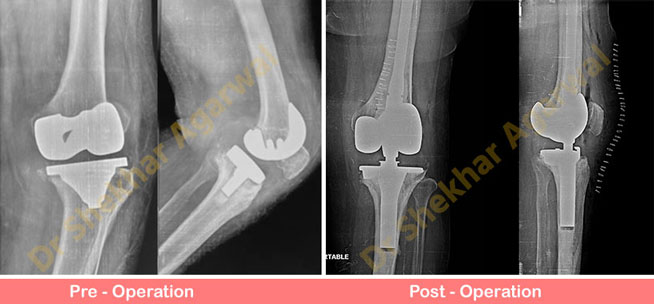
74 years old lady came with complaints of pain in left knee and difficulty in bearing weight over left lower limb for the past 6 months. She had undergone bilateral knee replacement 2 yrs ago. She fell 6 months ago and sustained a fracture of the proximal tibia which resulted in varus deformity and loosening of the tibial component. There was no evidence of infection. We planned for revision knee replacement with rotating hinge knee prosthesis. These surgeries require meticulous preoperative planning in terms of minimizing bone loss during prosthesis removal, reconstruction of the bone defect and inserting hinged knee prosthesis to overcome the instability due to insufficient ligaments. Post-operative x-ray showed RHK with wedge under tibial side to build up the medial defect. Now patient is comfortably bearing weight and walking with support.
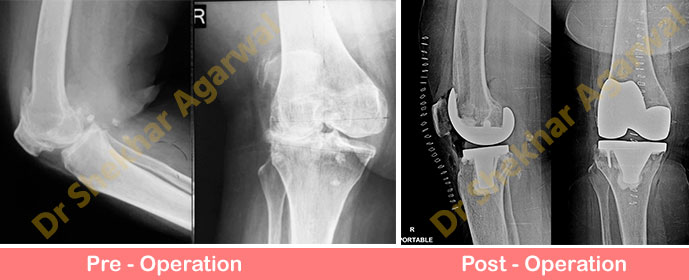
60 years old lady had difficulty in walking. She had osteoarthritis of right knee with valgus deformity. On examination the knee had fixed valgus and flexion deformity and painful range of motion.
These cases require meticulous planning and soft tissue releases to balance the knee than the usual varus OA knee. There is also increased risk of maltracking of patella and peroneal nerve palsy.
We did Total Knee Replacement using posterior stabilized primary knee implant. We recommend that constrained knee implants should always be kept as backup when operating such cases. Post op xray showing well balanced and aligned knee with knee prosthesis. The patient is comfortable after surgery and walking independently.
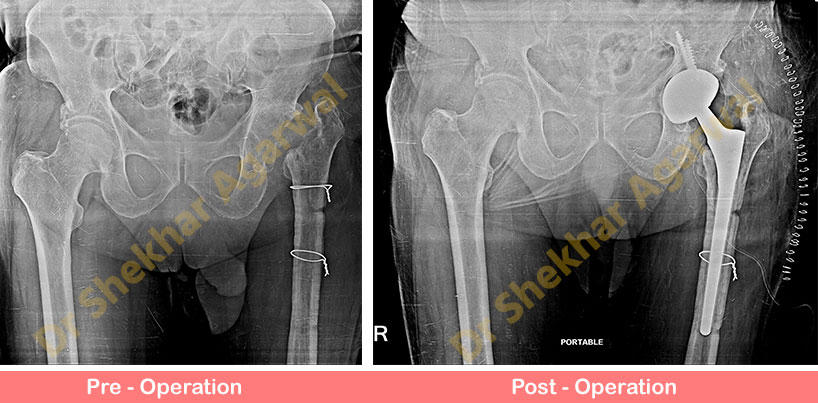
62 years old gentleman came with complaints of unstable left hip with difficulty in walking and shortening. He had undergone partial cemented replacement of the left hip in 2018. Subsequently he developed infection in this hip for which the hip prosthesis was removed and it was left as girdle stone. Preoperative X-Rays showed proximally migrated hip with shortening. Clinically there was no infection and blood parameters were normal.
He was planned for hip replacement with dual mobility uncemented acetabulum to ensure stability and further risk of dislocation. Shortening was also overcome by using the adequate length of the neck in the stem. Post op X-Rays showed dual mobility uncemented THR with long wagner stem to by pass the visible fracture line. Now patient is comfortable and walking with support.