Due to the sad demise of our beloved Dr.Shekhar Agarwal, his dedicated team of surgeons will be available for all your needs, please click on the below surgeon links to book an appointment with them
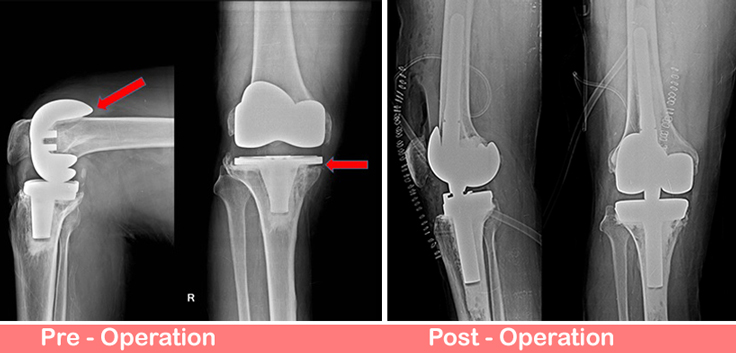
66 years old gentleman underwent bilateral Total Knee Replacement (Right 12 years and left 5 years back ) done elsewhere. He presented with complaints of instability, pain and difficulty in walking on the right knee. On Clinical examination there was effusion in right knee with instability. Infection markers were found to be normal and synovial fluid examination showed no evidence of infection. X-Ray was suggestive of aseptic loosening of tibia and femur.
We did revision Total Knee Replacement with Rotating Hinge knee. Both the femoral and tibial components were loose with extensive osteolysis of the femur and tibia. There was no clinical evidence of infection. Patient made satisfactory post-operative recovery.
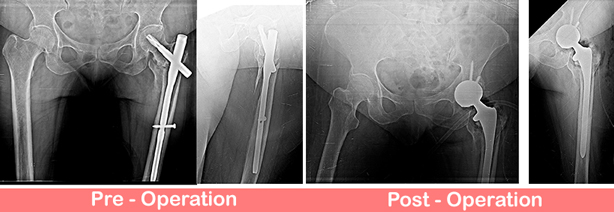
66 years old lady presented with pain, limp and inability to bear full weight over left lower limb for the past 1 year.
Patient had history of surgical intervention done elsewhere in view of proximal femur fracture 1 year back. Fracture was fixed with short PFN A2. Surgical site has been healed with primary intention and has no sign of infection. Her blood investigations were also come to be within normal limits.
Present X-Ray showing non union fracture proximal femur with Failed PFN in situ.
Thus planned for PFN removal and conversion to UNCEMENTED (DUAL MOBILITY) THR with long stem to bypass the distal screw.
Post op showing well press fit uncemented Total Hip Replacement (THR) with dual mobility cup to enhance the stability. These cases are challenging due to presence of ununited fracture in proximal femur and needs extra care for stability. We routinely do these cases with good outcomes using special dual mobility cup concept.
Now patient is happy, walking comfortably with support.
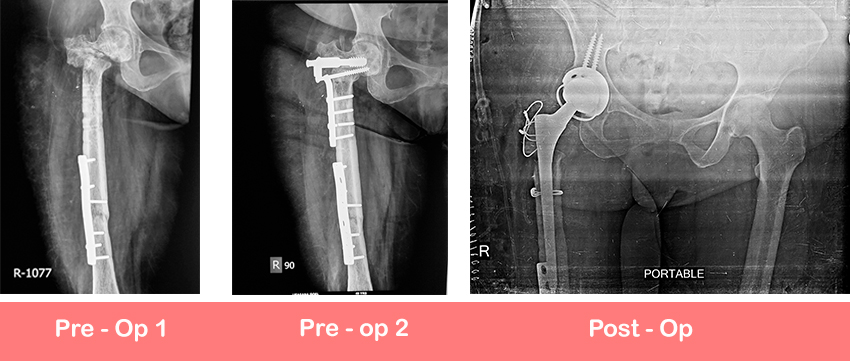
50 years lady presented with history of multiple times surgically intervened ipsilateral fracture neck of femur and shaft of femur right lower limb. She presented to us with complaints of pain in right hip region and difficulty in bearing full weight on right leg.
Present xray showed united fracture shaft of femur with plate in situ and nonunion osteotomy site with plate in situ
We did uncemented dual mobility constrained cup with long stem Total Hip Replacement