Due to the sad demise of our beloved Dr.Shekhar Agarwal, his dedicated team of surgeons will be available for all your needs, please click on the below surgeon links to book an appointment with them
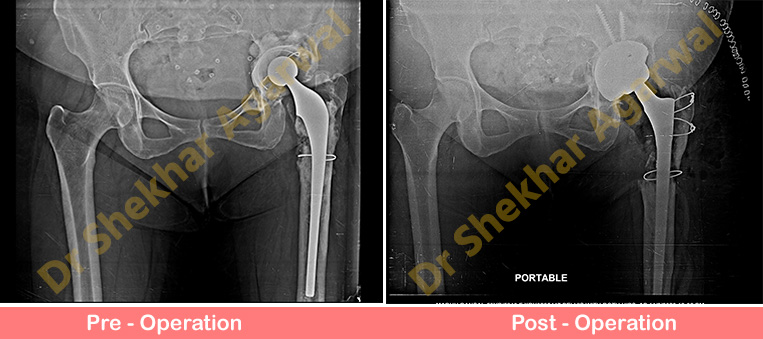
55 years old lady came to us with complaints of left hip pain and difficulty in bearing weight on left lower limb for the past 3 months. She underwent hip replacement surgery (THR) in 1995 followed by revision THR (2000 & 2008) elsewhere. On Clinical examination there were no signs of infection. There was shortening of 4 cm on left side.
Infection markers were negative. Preoperative x ray showed aseptic loosening of both acetabular socket and femoral stem. There was huge defect in acetabulum.
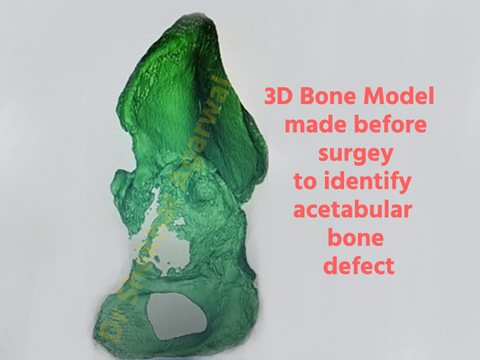
We further evaluated this case with CT scan which showed large anterior and superior bone defect while the posterior bone stock was good. We also prepared a 3D model of acetabulum preoperatively to study the defect and procure all the implants as backup for filling the defect. This 3D model was made under the guidance of Dr Shekhar Agarwal and team.
3D printing is the latest technology in Orthopaedics where we can have actual 3D model of bone and plan our surgery accordingly. 3D model exactly replicates actual bone defects which helps the surgeon to plan the surgery.
At Sant Parmanand Hospital we have this facility of 3D printing that we use in cases of difficult surgeries. As per our preoperative planning we did revision Total Hip Replacement (THR). Allograft bone was used to fill the acetabular defect and Trabacular metal jumbo acetabular cup was used. Uncemented long stem Wagner femoral stem was used on the femur. Now patient is comfortable and walking with support.
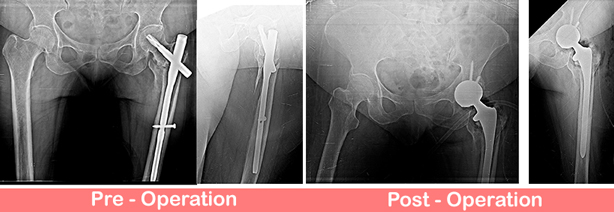
66 years old lady presented with pain, limp and inability to bear full weight over left lower limb for the past 1 year.
Patient had history of surgical intervention done elsewhere in view of proximal femur fracture 1 year back. Fracture was fixed with short PFN A2. Surgical site has been healed with primary intention and has no sign of infection. Her blood investigations were also come to be within normal limits.
Present X-Ray showing non union fracture proximal femur with Failed PFN in situ.
Thus planned for PFN removal and conversion to UNCEMENTED (DUAL MOBILITY) THR with long stem to bypass the distal screw.
Post op showing well press fit uncemented Total Hip Replacement (THR) with dual mobility cup to enhance the stability. These cases are challenging due to presence of ununited fracture in proximal femur and needs extra care for stability. We routinely do these cases with good outcomes using special dual mobility cup concept.
Now patient is happy, walking comfortably with support.
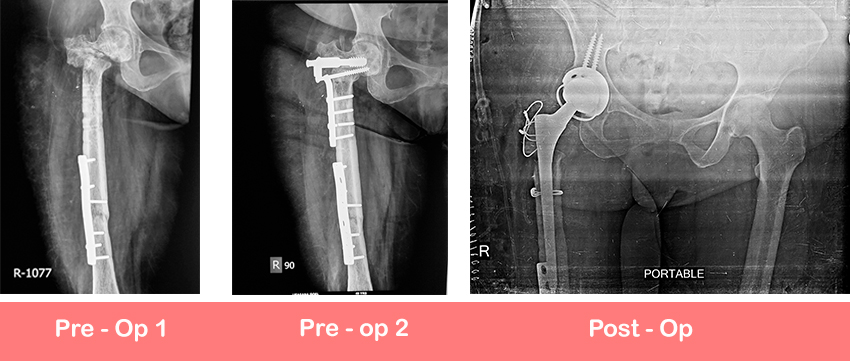
57 year old gentleman came to us with complaints of pain in right hip region and inability to walk and bear weight over right lower limb. Patient had past history of trauma to right hip region in the form of fracture acetabulum for which patient underwent primary fixation and Total Hip Replacement elsewhere in 2018. Subsequently patient developed dislocation of right Total Hip Replacement (THR) and underwent revision of acetabulum constrained component at our institute. Patient developed surgical site infection and re-dislocation of previously done hip and came to us for further management. Pre-op X-Ray pelvis with both hip joints showed dislocated hip with implant in situ
Patient planned for meticulous debridement and definite management for recurrent dislocation of hip. These complex cases required appropriate surgical planning and special surgical instrumentation. Because of previously done multiple surgeries leads to laxity of soft tissues and increases the risk of infection. This patient underwent thorough surgical site debridement to wash out the infection and one stage re-revision Total Hip Replacement (THR) was done using cemented constrained acetabulum. The femoral stem was also revised to a cemented stem.
50 years lady presented with history of multiple times surgically intervened ipsilateral fracture neck of femur and shaft of femur right lower limb. She presented to us with complaints of pain in right hip region and difficulty in bearing full weight on right leg.
Present xray showed united fracture shaft of femur with plate in situ and nonunion osteotomy site with plate in situ
We did uncemented dual mobility constrained cup with long stem Total Hip Replacement
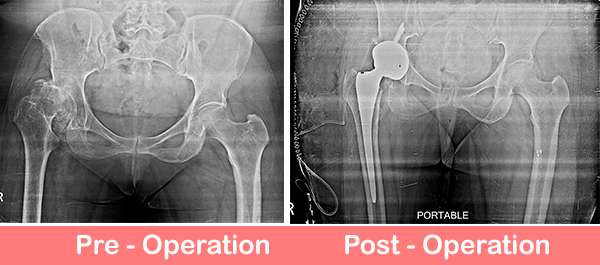
60 years female presented to the OPD with progressively increasing pain and limp right hip region for the past 2 yrs.
On examination she had severe deformities of the hip with 3 cm shortening. She was barely able to walk without support
Radiographs showed secondary OA right hip (severe dysplasia)
Management of dysplastic hip is tricky as locating true acetabulum in these cases can be difficult and challenging. Also soft tissue are severely contracted and there is alteration in the morphology of femur & acetabulum. We have done Uncemented Total Hip Replacement with acetabulum at anatomical position which requires expertise.
Now patient is walking comfortably with walker and without limp.

 55 years old lady came to us with complaints of left hip pain and difficulty in bearing weight on left lower limb for the past 3 months. She underwent hip replacement surgery (THR) in 1995 followed by revision THR (2000 & 2008) elsewhere. On Clinical examination there were no signs of infection. There was shortening of 4 cm on left side.
55 years old lady came to us with complaints of left hip pain and difficulty in bearing weight on left lower limb for the past 3 months. She underwent hip replacement surgery (THR) in 1995 followed by revision THR (2000 & 2008) elsewhere. On Clinical examination there were no signs of infection. There was shortening of 4 cm on left side.